Eating Disorders: Hypothalamic Reward Disruption and the Starvation Loop
Anorexia nervosa is not a choice — it is a disorder of the hypothalamic dopamine reward circuit in which restriction becomes neurologically reinforcing. Five people who broke the starvation loop through metabolic intervention.
TL;DR
Hypothalamic reward disruption, leptin/ghrelin dysregulation, DA reward hijacking. Stable ketone supply removes starvation-dependent reward. Five cases: adolescent AN, binge-purge, anxious AN, atypical male, ARFID.
The physiology
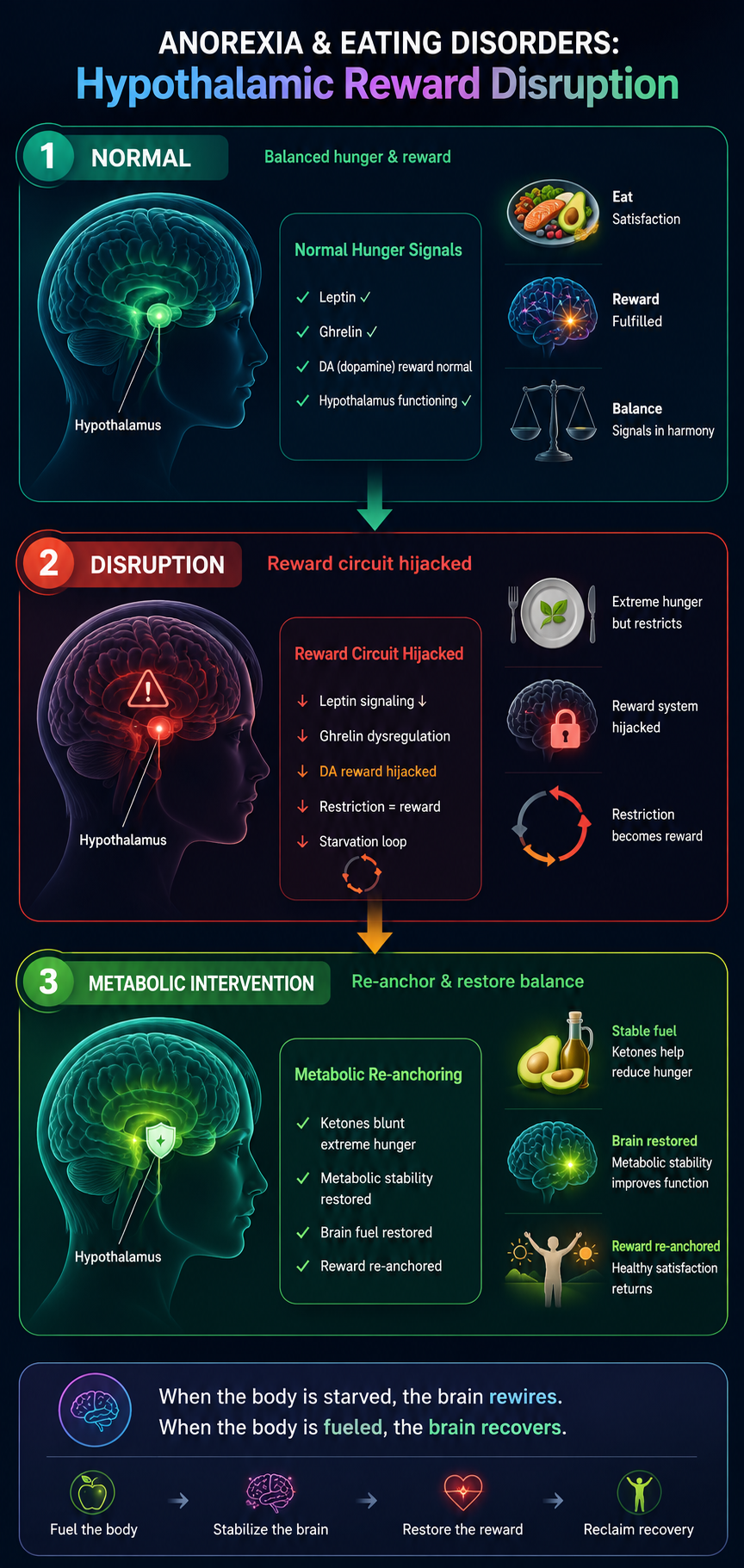
Anorexia nervosa is not a choice about aesthetics — it is a disorder of the hypothalamic reward circuit in which food restriction becomes neurologically reinforcing. Starvation in the context of anorexia produces a paradoxical neurochemical state: elevated dopamine in the reward pathway, increased physical activity drive, and suppression of normal hunger signalling through leptin and ghrelin dysregulation. The brain in a state of starvation runs on ketones produced from body fat — and in anorexia this state becomes self-perpetuating, because the ketotic state itself is experienced as rewarding.
The therapeutic insight is to provide exogenous ketones or a controlled ketogenic diet that maintains brain fuel supply without requiring the starvation-dependent dopamine reward. Clinical work by researchers including Dr. Guido Frank has documented abnormal reward circuit activity in anorexia patients; metabolic interventions target this circuit at its energy source rather than through behavioural intervention alone, which has a high relapse rate.
Five stories
Claire — Adolescent anorexia nervosa
Claire, 17, had anorexia nervosa severe enough to require hospitalisation for medical stabilisation. Refeeding with standard hospital nutrition was met with extreme distress. Her treatment team introduced a modified approach using ketogenic macronutrients — high fat, moderate protein — that provided sufficient energy without triggering the insulin surge associated with carbohydrate refeeding syndrome. The transition was markedly less distressing. She completed residential treatment and has maintained recovery for eighteen months.
Sasha — Binge-purge type
Sasha, 24, oscillated between restriction and binge-purge cycles — a pattern her therapist attributed to the neurochemical crash following periods of ketosis-induced restriction. When she adopted a stable low-carbohydrate eating pattern that maintained mild nutritional ketosis without severe restriction, the binge-purge cycle became less frequent. Her hypothesis, which her treatment team found plausible, was that the stable ketone supply removed the neurological desperation that drove the binge.
Lena — Anorexia with comorbid anxiety
Lena, 21, had anorexia with severe comorbid anxiety — the two conditions fed each other, with food restriction relieving anxiety temporarily while worsening it structurally. Her metabolic assessment found extremely low leptin and elevated cortisol. A structured nutritional rehabilitation programme using ketogenic macros stabilised her cortisol within eight weeks. As the anxiety diminished, the restriction drive weakened. She describes the sequence as logical in retrospect: the anxiety was metabolic before it was psychological.
Miles — Atypical anorexia in a male patient
Miles, 28, had atypical anorexia — clinically significant restriction and distorted body image without the low body weight that typically triggers treatment referral. His case was missed for four years. When eventually identified and treated, his metabolic workup showed severe mitochondrial dysfunction markers. Ketogenic nutrition plus structured refeeding produced metabolic normalisation over six months. His case highlights the importance of metabolic assessment in eating disorders regardless of body weight.
Tara — Avoidant-restrictive food intake disorder
Tara, 14, had ARFID — food avoidance driven not by body image but by sensory sensitivity and fear of choking. Her restricted diet had produced nutritional deficiencies that worsened her anxiety and sensory processing. A carefully structured nutritional intervention focused on metabolic adequacy first. As her brain nutrition improved — particularly omega-3 and fat-soluble vitamin status — her sensory sensitivity and food-related anxiety both diminished, expanding the range of foods she could tolerate.