Multiple Sclerosis: The Immune System Strips Nerve Insulation
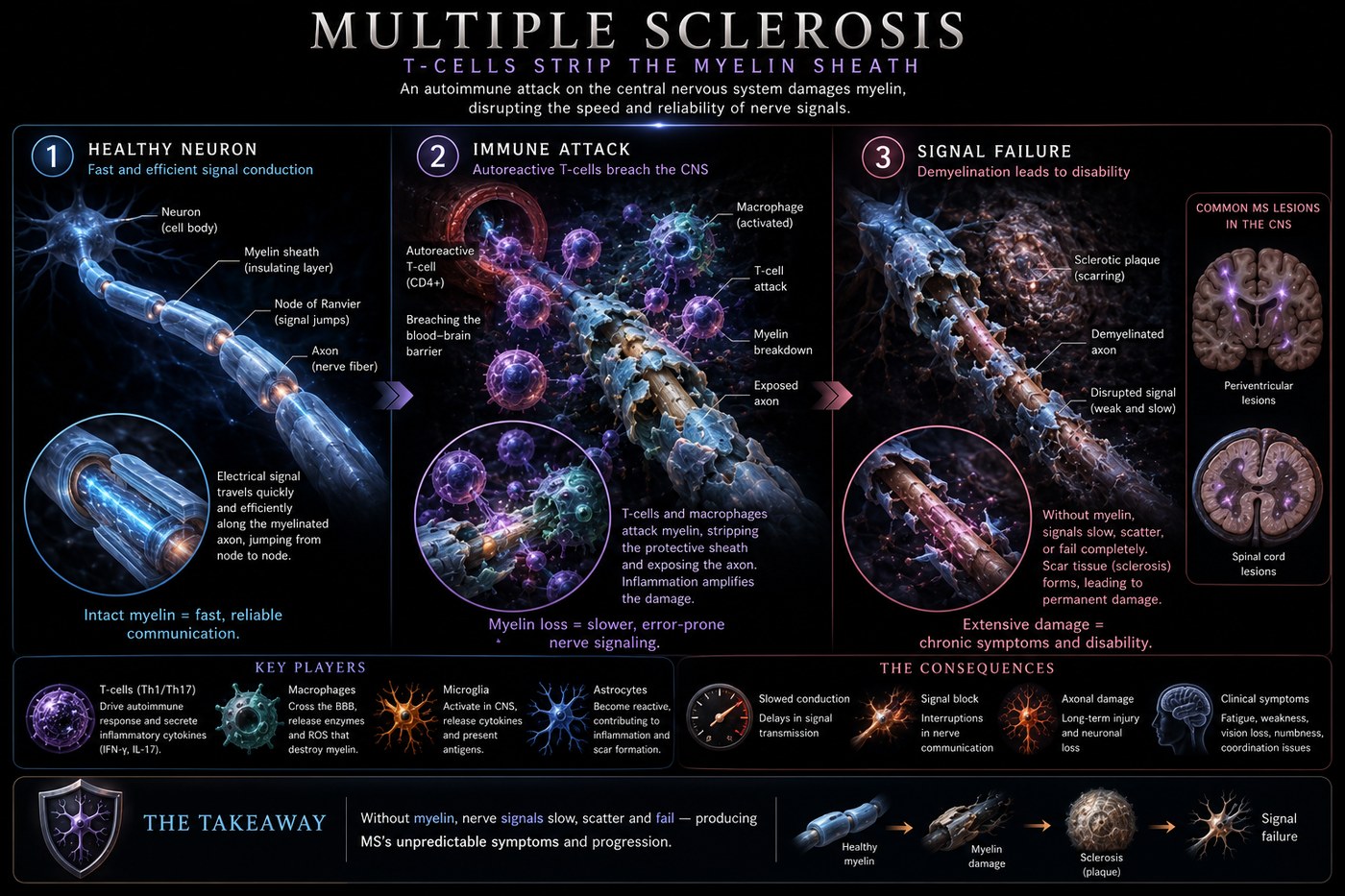
In multiple sclerosis, autoreactive T-cells cross the blood-brain barrier and destroy myelin — the insulating sheath around nerve fibres. Without myelin, electrical signals slow, distort, and eventually fail, producing the cascading neurological deficits of the disease.
What is happening in the body
The central nervous system is normally protected from immune surveillance by the blood-brain barrier — a tightly sealed endothelium that prevents most immune cells from crossing into brain tissue. In MS, that barrier fails at focal points. Autoreactive CD4+ and CD8+ T-cells — primed in the periphery to recognise myelin antigens, particularly myelin basic protein (MBP) — cross into the CNS and initiate an inflammatory cascade.
The T-cells attack the myelin sheath, the fatty insulating layer wrapped around axons by oligodendrocytes. Myelin is not decorative — it enables rapid saltatory conduction, the mechanism by which electrical signals jump between nodes of Ranvier at high speed. When myelin is stripped, conduction slows dramatically. In areas of complete demyelination, transmission fails entirely. Repeated episodes of inflammation leave behind glial scars — the "sclerotic plaques" that give the disease its name — which resist remyelination.
The location of each plaque determines the symptom. Lesions in the optic nerve cause visual disturbance. Lesions in the spinal cord cause limb weakness and bladder dysfunction. Lesions in the cerebellum cause balance problems. Over time, progressive axon loss — even in areas with incomplete demyelination — produces the irreversible neurological decline of secondary progressive MS.
The symptoms this produces
- Optic neuritis — blurred or lost vision in one eye, often painful
- Numbness, tingling, or electric sensations in limbs (Lhermitte's sign)
- Muscle weakness and spasticity
- Fatigue disproportionate to activity
- Bladder urgency and incontinence
- Cognitive difficulties — memory, processing speed
- Balance and coordination problems (ataxia)
How this fits the autoimmune pattern
The peripheral priming of myelin-reactive T-cells almost certainly requires an environmental trigger. Molecular mimicry between bacterial or food peptides and myelin antigens is the most studied mechanism. Wheat gliadin shares peptide sequences with MBP; dietary lectins and gut dysbiosis create the systemic immune activation that allows autoreactive clones to escape tolerance. Epidemiological studies show MS prevalence tracking closely with wheat consumption and latitude-based vitamin D deficiency — both downstream effects of the same dietary and lifestyle variables that drive intestinal permeability.
What the clinical data shows
Paleomedicina case series include patients with relapsing-remitting MS who achieved sustained remission — no new MRI lesions, no clinical relapses — on the PKD protocol. In several cases, patients who had been on disease-modifying therapy (interferon beta, glatiramer acetate) were able to taper and discontinue medication under clinical supervision after MRI stability was established. The PKD's elimination of gluten, dairy, and processed foods removes the peripheral antigenic triggers while the animal-fat-rich diet provides the cholesterol and saturated fatty acids required for myelin synthesis and repair.
A life with this condition — Stories
James, 31. He noticed something wrong when his right foot stopped lifting properly on long runs. By the time he saw a neurologist six weeks later, his right leg felt wrapped in cotton wool and his left eye had given him a week of blurred vision he had attributed to fatigue. The MRI showed nine lesions scattered through the white matter of his brain and along his cervical spine. He was diagnosed with relapsing-remitting MS on a Thursday, sat in the car for an hour unable to drive, and spent the next year learning why rest reliably restored function that exercise took away, and why heat made everything worse.
Rachel, 27. Her first symptom was pain behind her right eye, followed within days by a grey smear across the centre of her vision. Her optometrist referred her urgently; her ophthalmologist said "optic neuritis" within the first minute of the examination. The neurology referral happened the same day. Her MRI showed two lesions in the white matter — not enough for an MS diagnosis yet, but enough to call it clinically isolated syndrome, which her neurologist explained carried a 50% risk of a second episode within two years. Thirteen months later, she had the second episode. The diagnosis became definitive.
David, 44. His MS crept in without drama. There was no single devastating episode — just a gradual narrowing of what his body could do. He had begun to notice fatigue so disproportionate to his activity that he stopped mentioning it socially, because no one had a frame of reference for exhaustion that arrived after a short walk. He was eventually diagnosed with primary progressive MS, the form that accumulates disability steadily without distinct relapses. His MRI showed lesions that had been there, silently, for years. There had been no acute event to send him to a doctor sooner.
Simone, 36. Her MS diagnosis came only after she pushed back on a psychiatry referral. She had double vision and left-sided numbness; her first neurologist attributed both to stress and anxiety. She came prepared to her second appointment with a printed list of her symptoms, their timings, and the Lhermitte's sign she had looked up herself — an electric shock sensation down her spine when she flexed her neck. An MRI the same week showed seven lesions. She had been right. The cost of the three-month delay between appointments was one relapse.
Transcript witness — Dr. Anthony Chaffee podcast. A practitioner who has documented MS patients improving on carnivore: "I have a patient — not a patient of mine, but someone I have discussed for our case series — who is reversing multiple sclerosis on an animal-based diet. When you remove the things that are causing the damage, the body is very good at repairing itself. Myelin can remyelinate. It is not fast, but it happens. The key insight from the Epstein-Barr research is that MS is probably not a disease of the nervous system generating its own attack — it is the immune system responding to a viral trigger that it cannot resolve."
Kieran, 29. He was a professional cyclist when his first relapse took his right leg's coordination. He spent two months in physiotherapy recovering what the demyelination had taken. He returned to racing; his neurologist put him on a disease-modifying drug that reduced relapse rate but produced fatigue that made competitive racing impossible. He retired from professional sport not because of the MS directly but because the medication required to control it took away what the disease had not. He described the trade-off as "choosing which kind of loss to live with."
Beatriz, 52. She had been in clinical remission on natalizumab for six years when her neurologist raised the concern of PML — a rare but often fatal brain infection that becomes a risk after extended natalizumab use in JC virus-positive patients. She tested positive for JC antibodies and needed to switch medication. The switch triggered a rebound inflammatory activity that produced her worst relapse in a decade. Her neurologist had warned her this could happen; knowing it was possible had not prepared her for the reality of losing two weeks of mobility while her new drug established effect.
Anthony, 44. His transition from relapsing-remitting to secondary progressive MS happened without a distinct moment — just a gradual understanding, over eighteen months of monitoring MRI scans that showed no new lesions but a slow, steady loss of walking distance, that the character of his disease had changed. His neurologist explained the distinction: in the relapsing phase, relapses are the main driver of disability; in progressive disease, it is slow neurodegeneration that continues independently of inflammation. The drugs that had worked before were now addressing the wrong mechanism. Treatment needed to change.