Psoriasis: The Skin That Cannot Stop Growing
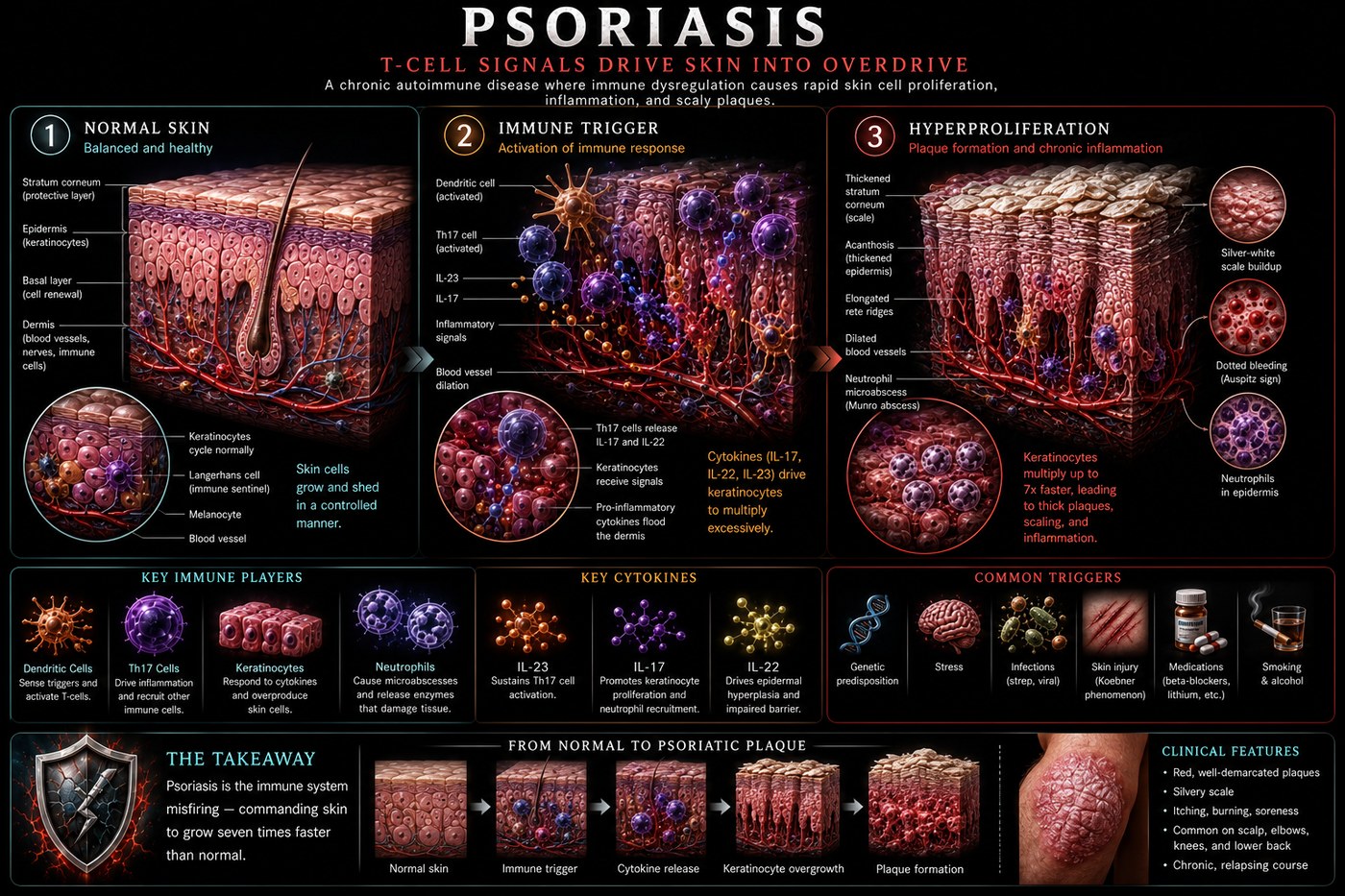
Psoriasis is driven by IL-17 and IL-23 cytokines that lock the skin into a state of hyperproliferation. Keratinocytes that normally renew over 28 days complete the cycle in 3–4 days, piling up as the characteristic silver-scaled plaques of the disease.
What is happening in the body
Psoriasis begins not in the skin but in the dendritic cells of the dermis. Plasmacytoid dendritic cells, activated by self-DNA or microbial triggers, produce interferon-alpha and IL-12/IL-23. IL-23 drives the differentiation of naive T-cells into Th17 cells, which secrete IL-17A, IL-17F, and IL-22. These cytokines act on keratinocytes — the cells that form the skin's outer layers — and trigger a profound shift in their behaviour.
Normal keratinocytes in the epidermis take approximately 28 days to mature, migrate from the basal layer to the surface, and shed. Under sustained IL-17 stimulation, that cycle compresses to 3–4 days. The hyperproliferating keratinocytes do not have time to mature properly — they retain their nuclei (parakeratosis) and pile up in the characteristic silvery scale above the inflamed dermis. The dilated, tortuous capillaries of the dermal papillae produce the punctate bleeding (Auspitz sign) when scale is removed.
The symptoms this produces
- Well-demarcated, raised plaques with silvery-white scale on elbows, knees, scalp, lower back
- Itching, burning, soreness at plaque sites
- Nail changes: pitting, onycholysis, oil-drop discolouration
- Psoriatic arthritis in 20–30% of patients (can be erosive)
- Koebner phenomenon: new plaques appearing at sites of skin trauma
- Significantly elevated cardiovascular disease risk (shared inflammatory terrain)
How this fits the autoimmune pattern
Psoriasis flares reliably following gut dysbiosis events — antibiotic courses, gastrointestinal infections, alcohol excess. Streptococcal pharyngitis triggers guttate psoriasis in children through molecular mimicry between streptococcal M-protein and keratin. The same gut permeability mechanism that drives other autoimmune conditions creates the systemic IL-23 and IL-17 dysregulation that characterises psoriasis. Patients with psoriasis have measurably increased intestinal permeability compared to controls.
What the clinical data shows
Case reports and series document dramatic clearance of psoriatic plaques on the PKD, with some patients achieving complete skin clearance within weeks of eliminating grains, legumes, and processed foods. The mechanism is dual: removal of the gut permeability drivers that fuel the IL-23/Th17 axis, combined with the direct anti-inflammatory effect of ketone bodies on NLRP3-mediated IL-1 and IL-18 release. Psoriatic arthritis has shown parallel improvement in the same patients, confirming shared upstream drivers.
A life with this condition — Stories
Amara, 22. She noticed the first plaques on her elbows and waited three months before seeing a doctor, embarrassed by what they looked like. By then her scalp was involved and she was wearing her hair differently to cover the scale at her hairline. What her dermatologist showed her on a diagram changed how she thought about it: normal skin renews in 28 days; her affected patches were completing that cycle in three. The IL-17 flooding her dermis had locked her keratinocytes into a proliferation they could not stop. The scale was the skin's failed attempt to shed what it was producing too fast to control. Understanding this did not make it less visible. But it made it less shameful.
James, 35. His psoriasis arrived two weeks after streptococcal tonsillitis — hundreds of small teardrop-shaped spots across his trunk and limbs almost overnight, the guttate pattern that follows streptococcal infection in susceptible people. His GP diagnosed it immediately. The bacterial M-protein had triggered a T-cell response that cross-reacted with keratin in his skin; his immune system had learned to attack his own skin surface while fighting an infection in his throat. Most guttate episodes clear within months. His did not fully clear; it evolved into chronic plaque psoriasis, as if the infection had unlocked something that could not be fully locked again.
Rosa, 48. She had managed her psoriasis for twenty years with topical treatments when her fingers began swelling at the joints in a pattern her rheumatologist recognised immediately as psoriatic dactylitis — "sausage fingers," where the entire digit swells because both the joint and the tendon sheath are inflamed simultaneously. Her nail pitting had been present for years; she had not known it was a marker of joint involvement risk. Twenty percent of psoriasis patients develop psoriatic arthritis, and the skin disease almost always precedes the joint disease by years. She had been carrying a warning in her fingernails for a decade without anyone reading it.
Transcript witness — Dr. Anthony Chaffee podcast. A speaker describing her daughter's psoriasis remission: "My oldest daughter has severe psoriasis and was on biologics. You can't tell your kids anything, really. But she is off the medication. She is not fully carnivore, but she is on a strict ketogenic diet and weight training, and she has been off her biologics for nine months. Biologics are dangerous drugs — serious side effects, serious long-term risks. The idea that a dietary change could get someone off them, without a drug company funding the trial, means no one is studying it properly. We are living the study."
Transcript witness — zerocarb community. Wendy, medical herbalist: "I have had chronic scalp psoriasis for years. After trying broccoli — I had been 99% carnivore for two years — I started itching my scalp again. I thought, 'Wow, I had not had that. I had not noticed it gone until it came back.' That is how you discover something is a trigger. You only see the absence when you reintroduce. The carnivore community is full of people who discovered this the same way: something came back, and then they knew."
Callum, 44. His psoriasis had covered thirty percent of his body surface area at its peak and he had been through methotrexate, acitretin, and two biologics. He had not been told, in ten years of dermatology appointments, that there was any meaningful dietary approach worth considering. He found a carnivore community online, tried it for ninety days, and experienced the most significant skin clearance of his adult life. He went back to his dermatologist with photographs. His dermatologist said it was probably a spontaneous remission. He asked whether it was possible the diet had caused it. His dermatologist said: "I couldn't say either way." Callum stopped the diet. The plaques returned within three weeks. He went back to the diet. His dermatologist had no comment.
Nora, 19. Her guttate psoriasis appeared two weeks after a strep throat infection — hundreds of small teardrop spots covering her trunk, back, and upper arms almost overnight. Her GP identified it immediately and told her that guttate psoriasis following strep infection was a well-recognised pattern. What her GP also told her was that most guttate episodes resolve within three to four months. Hers did not. At six months it had evolved into plaque psoriasis. Her GP referred her to dermatology. The infection had been the trigger. The genetic susceptibility had been there all along. The infection had just unlocked something that could not be fully closed again.
Theo, 56. He had psoriasis for thirty-one years and had accepted it as a chronic condition he managed rather than one he could change. What shifted his thinking was a cardiac event — a heart attack at 54 — that his cardiologist attributed partly to the chronic systemic inflammation of longstanding psoriasis. He had not known that psoriasis significantly elevated cardiovascular risk independent of traditional risk factors. He had been treating his skin. His cardiologist was treating his arteries. Nobody had explained to him that the same inflammatory process was doing damage in both places simultaneously.